SkiaQA · The quality layer
A second set of eyes on every report.
SkiaQA reviews every report against your clinical consistency rules before it submits. The errors your QA process is trying to catch stop reaching your clients.
Every check runs while the report is being finalized. The flag is fixed before submit, not after a callback.
- Every report, not a sample
- Before submit, not after a callback
- A handful of flags, not a wall of warnings
- Zero patient data stored by Skia

01Why this exists
Manual QA is inconsistent by nature
Right now there is a QA process somewhere in your operation. A second reader. A coordinator with a checklist. A pass before reports go out. It costs time, it costs money, and it still misses things.
Not because nobody was trying. The errors that reach your clients did not slip through by accident. They slipped through because no human process catches everything, every time, on every report, at 2am as reliably as at 10am.
SkiaQA does not get tired, distracted, or behind on volume. It applies the same checks to the first report of the day and the four hundredth.
Radiology error rates run 3 to 5 percent in daily practice (Brady, Insights into Imaging, 2017). A 5 percent peer review sample is the accepted industry standard (ACR RADPEER; Royal College of Radiologists).
02What it checks
The checks a tired reader misses
Every report is read against the same set of clinical consistency rules. Here is what that covers today, and the list keeps growing. Flags are ranked by severity, so a laterality contradiction never reads like a spelling slip.
Critical
Laterality
Catches a right finding written into a left section, or sides that contradict between findings and impression.
Critical
Critical findings
Highlights findings that need to be communicated, so nothing urgent leaves quietly buried in the body.
Clinical
Comparison dates
Flags a missing prior, the wrong prior, or a comparison date that does not match the study being read.
Clinical
Internal contradictions
Surfaces statements that disagree with each other inside the same report before they reach a clinician.
Clinical
Findings and impression
Confirms the impression actually reflects the findings, with nothing significant left unaddressed.
Clinical
History and technique
Checks that the clinical history and technical factors are present and consistent with the findings.
Polish
Grammar and spelling
Cleans the language errors that make a report read as rushed, without changing its meaning.
Polish
Completeness
Verifies every required section is filled in for the modality and body part being reported.
03One report, one card
What a finished review looks like
Every report leaves with its review on record: each check that ran, what passed, and what was flagged with the exact reason. The mismatched side, the stale comparison date, the missing impression. Then a summary, a quality score, and a clean ready to sign.

04How it works
A quality gate that is always on
-
It runs on every report
Not a weekly sample, not a second reader for the high risk cases. Every report your team produces is reviewed the same way, every time.
-
It checks before submit
The review happens while the report is being finalized, in seconds. Issues are caught before the report leaves, not after a hospital client calls back.
-
The radiologist sees the flags
Problems show up inline for the person who can fix them fastest. Fix once, submit clean. Most flags are resolved in the moment, without a single email.
-
You get told what matters
QA flags and critical findings can notify you and your team, so you have visibility without reading behind every radiologist.
The gate is always on. Nobody schedules it, nobody samples it.
05The QA worklist
Reports written anywhere, triaged in one list
Your radiologists do not have to report in Skia. Point SkiaQA at the worklist and it works through every study on its own, reads each finished report wherever it was written, and marks the record with a clean tick or a flag.
Fifty studies in, a handful that need a person. The list arrives already triaged.
It reads the whole list
A worklist of fifty studies means fifty reports read, automatically, as they are finalized. Nobody assigns QA work and nothing waits for a sampling schedule.
Any editor, including dictation
This is how SkiaQA covers reports produced outside Skia. Dictated, typed, or assembled in the tool your team already uses, the finished text is what gets checked.
Triage for the person who owns quality
Clean reports get a quiet tick. Flagged ones show what was found right on the row, so your QA lead opens only the records that need attention instead of reading one by one to find out.
Flags can notify
With SkiaManager alongside, a flagged record reaches the right person on the channels your team already uses. On its own, the list itself is the triage.
06What changes for you
You stop being the last line of defense
Volume can grow without growing the people you pay to re-read reports that were already fine.
A night shift, drawn to scale: 200 reports, 200 reviews, 8 flags caught before they shipped. The 2am report gets the same scrutiny as the 10am one. Illustrative.
- Every
- Report checked before submit
- Fewer
- Callbacks from clients
- One
- Standard applied to all
- Zero
- Patient data stored by Skia
Results vary by case mix, modality, and team. Overnight reads show higher discrepancy rates for residents and attendings alike (Radiology, 2020). The rules do not get tired.
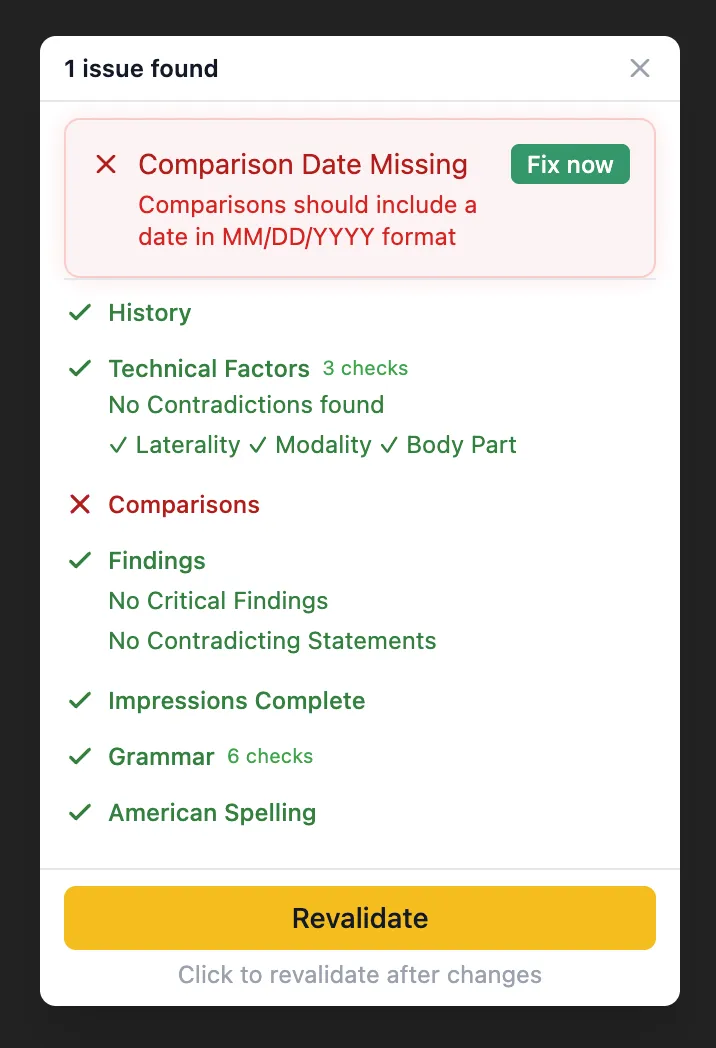
The actual panel your radiologists see. One issue, one fix, submitted clean.
07For the department head
The business case, in three numbers
You do not need radiology training to weigh a quality layer. The case translates into the two currencies every administrator already counts: hours and liability.
What slips through
71%
of addenda were fixing real errors
A review of 97,003 finalized reports at one high volume center found that when an addendum was issued, 71 percent of the time it was correcting a real error: a missed finding, a wrong interpretation, a communication slip. Every one was caught after the report had already shipped.
What one error costs
£1.85M
paid by one NHS trust in five years
27 imaging negligence claims cost a single UK trust £1.85 million, about $2.4 million, between 2020 and 2025. English trusts have faced over 2,100 radiology negligence claims in that time. A flag fixed before submit never becomes a claim.
What a shift gets back
100 min
of clinical time recovered daily
Administrators plan in shifts, not reports. If catching issues inline saves each radiologist 20 minutes of callbacks and addenda per shift, a five radiologist roster recovers 100 minutes of clinical time every day.
Addenda data: Indian Journal of Radiology and Imaging, 2021, a 1.1 percent addenda rate across 97,003 cross sectional reports at a single center. Claims data: NHS Resolution figures reported in 2025, with the trust level payout from Worcestershire Acute Hospitals NHS Trust. Time per shift is illustrative and varies by case mix and volume.
08For the team running it
You cannot scale second reads.
You can scale the standard.
Doubling your QA coverage the manual way means doubling the people who re read reports that were already fine. SkiaQA applies one standard to every report from every radiologist, on every shift, in every time zone, without adding a single reader.
Volume can grow without growing the people you pay to re read reports. You stop being the last line of defense, because the line is built into the workflow.
09Common questions
Asked by every radiology team we meet
Does SkiaQA replace our peer review program?
It closes the gap peer review leaves open. Peer review samples a small share of reports weeks after they were sent, which is right for credentialing and learning. SkiaQA reviews every report before it submits, so errors are caught while they can still be fixed. Most teams keep both.
Will it flood radiologists with warnings?
No. Flags are ranked by severity and most reports pass clean. A laterality contradiction is treated very differently from a spelling slip, and the radiologist sees a handful of high signal flags inline, not a wall of warnings.
What exactly does it check?
Comparison dates, laterality, internal contradictions, history and technique, findings versus impression, critical findings, grammar and spelling, and completeness. Every report is read against the same set of clinical consistency rules, and the list keeps growing.
Do reports have to be written in Skia to be checked?
No. SkiaQA can run through your worklist and read finished reports wherever they were written, including dictated ones from the editor your team already uses. Each record gets a tick or a flag, so quality review starts from a triaged list instead of a pile of unopened reports.
Does it rewrite the radiologist's report?
No. SkiaQA flags issues and the radiologist decides. Problems show up inline for the person who can fix them fastest. Fix once, submit clean. The radiologist keeps the final say on every word.
Where does patient data go?
Your data never leaves your PACS. Skia stores zero patient data.
Can we use SkiaQA on its own?
Yes. SkiaQA works standalone. Every report is checked before it submits without SkiaReporter or SkiaManager in the picture. Start with the quality layer alone and add the rest of Skia when you are ready.
How long does it take to go live?
No setup fees, no IT project, no training required. Most teams are live within 48 hours.
10Further reading
Go deeper on the problems this solves
Who checks the AI in your radiology reports?
AI now drafts radiology reports faster than ever, but verification has not kept up. Why every AI-assisted report still needs a quality gate before sign-off.
Read articleCommon errors in radiology reports and how to stop them
Learn the common errors in radiology reports, why they reach clients, and how to catch laterality, contradiction, and communication issues before sign-off.
Read articleRadiology peer review vs automated QA in real practice
Compare radiology peer review and automated QA by timing, coverage, and value so you know which method prevents report defects and which improves learning.
Read articlePreliminary and final read discrepancy explained
Learn how to measure preliminary and final read discrepancy, what managers should track, and how to reduce avoidable corrections in outsourced workflows.
Read articleBuild a radiology QA program that scales with volume
Build a radiology QA program that scales with volume by separating clinical review from report checks, tracking the right metrics, and covering every report.
Read articleWhy Radiology QA Still Fails and What to Do About It
Most radiology QA catches errors only after they reach referring physicians. Why manual QA falls short, and how real-time automated QA protects your practice.
Read article11The rest of Skia
SkiaQA works standalone. Nothing here is required. Add either product when you are ready.
See what SkiaQA catches in your own reports
No setup fees, no IT project, no training required. Most teams are live within 48 hours.